
November 5, 2015 UPDATED – In the original post we mentioned that there was no published evidence demonstrating that the Inhibrx/Celgene CD47 antibody (CC-90002) does not induce RBC agglutination. This statement was factually incorrect. Mark Lappe, CEO of Inhibrx, was kind enough to reach out to us, pointing us to Inhibrx patent filings, where they demonstrate that CC-900002 does not cause RBC agglutination. See ‘The CD47 competitive landscape’ section for updated details. An additional hat tip to Dan Marks (@Festivus159) for also spotting our error.
November 4, 2015
Although they are still in early clinical development, therapeutic strategies aimed at targeting CD47 have the potential to be deployed in a broad range of oncology indications as a backbone of cancer treatment. As an investment thesis, Trillium Therapeutics (NASDAQ:TRIL) provides a compelling opportunity to own a biotechnology company singularly focused on CD47 as immuno-oncology target.
CD47 is a ‘don’t eat me’ signal

In order to distribute oxygen from the lungs throughout the body the average human requires on the order of twenty to thirty trillion red blood cells (e.g. 20-30,000,000,000,000 RBCs). Amazingly, ten billion RBCs are produced via erythropoiesis every hour. The rapid production of RBCs is due in part to a relatively short functional lifespan of approximately 120 days. Old and damaged RBCs are cleared from circulation in the spleen by macrophage-mediated phagocytosis (this process is depicted by a falsely colored electron micrograph in Figure 1). Although scientists have been aware of the process of RBC phagocytosis for many years, the molecular mechanism has remained elusive. Part of the puzzle was solved in 2000 when investigators hypothesized that CD47 served as a marker of ‘self’. More specifically, Oldenberg et al. proposed that surface expression of CD47 on RBCs served as a mechanism to prevent macrophage phagocytosis (Figure 2). This hypothesis was supported by experiments involving genetically engineered mice lacking the CD47 gene. Oldenberg and colleagues injected CD47 -/- RBCs into wildtype recipients and found that they were rapidly eliminated from circulation in these mice through splenic macrophage phagocytosis. Additionally, they demonstrated that the interaction between CD47 and its cognate binding partner SIRPα is important for this function. Engagement of SIRPα by CD47 results in phosphorylation of cytoplastmic SIRPα ITIM motifs, subsequent recruitment of SHP-1, and inactivation of actin cytoskeleton processes required for phagocytosis.

The dysregulation of CD47 expression in cancer
Cancer deploys a variety of methods to evade immune detection (written about previously here). To avoid detection and subsequent phagocytosis by macrophages, cancer cells upregulate CD47 expression on their cell surface (Figure 3). Since upregulation of CD47 is observed in nearly all solid and hematological malignancies it is likely a broadly conserved tumor escape mechanism. Figure 3 illustrates the expression level of CD47 on patient cells isolated from ovarian, breast, colon, bladder, glioblastoma, hepatocellular carcinoma, and prostate cancers relative to matched normal controls. On average, CD47 expression is increased in these solid tumor samples about 3 fold relative to matched normal cells. Similarly, cell surface CD47 upregulation is observed in patient cells isolated from hematological malignancies including non-hodgkin lymphoma, acute myeloid leukemia, and acute lymphoblastic leukemia. The disease-relevance of CD47 upregulation is illustrated by a striking correlation with clinical outcomes. Figure 4 demonstrates the prognostic value of CD47 expression across a number of solid and hematological cancers. In the examples illustrated, high CD47 expressing (‘CD47 high’) tumors have worse progression free survival and overall survival than their lower expressing (‘CD47 low’) counterparts. Although the relationship between high CD47 expression and clinical outcomes is correlative, from our understanding of tumor immunology, one could speculate that the high CD47 expression mediates immune evasion, resulting in a more aggressive tumor phenotype, which lends to the observed clinical outcomes.


Preclinical evidence demonstrating the efficacy of anti-CD47 strategies
The table in Figure 5 summarizes preclinical studies examining the efficacy of disrupting the CD47-SIRPα axis in hematological and solid malignancies. In the interest of both time and space we will refrain from commenting on every study, save a few compelling examples. The use of a CD47 monoclonal antibody in both an orthotopic breast cancer patient derived xenograft (PDX) (Figure 6) and an orthotopic ovarian PDX (Figure 7) result in complete regressions. In both cases blocking CD47 results in a remarkable and rapid tumor elimination via macrophage phagocytosis. Furthermore, Figure 8 and 9 demonstrate the effectiveness of targeting CD47 in glioblastoma and bladder cancer xenografts, respectively.





Anti-CD47 strategies can convert TAMs into a pro-phagocytic, anti-tumor phenotype
Leiomyosarcoma (LMS) is a tumor of the smooth muscle and is typified by the presence of tumor-associated macrophages (TAM). Not surprisingly, because of their pro-tumor and immunosuppressive function, the level of TAM infiltration in LMS is postively correlated with poor clinical outcomes. Primary LMS is commonly treated via surgical resection, but unfortunately the rate of metastatic relapse for these tumors following surgery is approximately 40%. Figure 10 illustrates the development of an aggressive neoadjuvant model of metastatic LMS using an LMS cell line and immunocomprimised mice. The use of a CD47 antibody in this setting is capable of converting resident TAMs from a pro- to an anti-tumor phenotype, resulting in the elimination of lung metastases (notice the lack of brown staining, indicative of metastatic tumor cells, in the lung section of a mouse treated with anti-CD47 in Figure 10). These data provide evidence to demonstrate the effectiveness of anti-CD47 strategies against metastatic disease, as well as the ability to convert immunosuppressive TAMs towards a phagocytic, anti-tumor phenotype.

CD47 combinations with targeted agents
In non-hodgkin lymphoma xenografts monoclonal antibodies against CD47 perform comparably to Rituximab (Figure 11). In fact, in this setting, both agents display somewhat lackluster efficacy. Compared to single agent efficacy in examples shown in previous figures, the anti-CD47 antibody does little to prevent tumor growth in this model. However, when Rituxmab is administered in combination with an anti-CD47 antibody there is marked synergy, and many of the mice exhibit durable complete responses. These data support the use of a potentially less toxic and chemo-free CD47/CD20 combination regimen for aggressive non-hodgkin lymphoma. Investigators have also combined anti-CD47 with alemtuzumab (anti-CD52) and although the combination is effective, it appears to be less spectacular than CD47/CD20.


Therapeutic index of anti-CD47 strategies depends on a balance of pro and anti-phagocytic signals
For cells of the body which routinely encounter macrophages, phagocytic homeostasis is maintained by a balance of pro and anti-phagocytic cell-surface signals. For example, CD47 is an anti-phagocytic signal, and is highly expressed in cancer — masking CD47 on the cancer cell surface results in phagocytosis and elimination. Interestingly, normal cells are largely unaffected by CD47 antibodies at concentrations high enough to induce phagocytosis of cancer cells (see Figure 13). In part, this is due to higher CD47 expression on tumor versus normal cells (recall the CD47 expression differential as shown in Figure 3). Although, perhaps more importantly, cancer cells also display various pro-phagocytic signals on their surface due to a high unfolded protein response, cell cycle deregulation, and accumulated DNA damage. One such pro-phagocytic signal is calreticulin. Calreticulin is a calcium sensing protein, which is typically bound to the endoplastmic reticulum, found on the inside of the cell. Due to the aforementioned stressors experienced by cancer cells the distribution of this protein becomes more diffuse and it begins to appear in the cell surface. In fact, calreticulin is highly expressed in cancers and its expression is highly correlated with CD47 expression — from an evolutionary perspective it’s possible that cancer cells increase CD47 level to compensate for stress-mediated calreticulin outer-membrane deposition. Tumor calreticulin cell surface expression is necessary for anti-CD47 antibodies to eliminate tumor cells. By masking surface calreticulin expression via a blocking peptide, investigators are able to abrogate anti-CD47-mediated phagocytosis (Figure 13). Thus the cancer-specific surface expression of calreticulin provides a rational mechanistic explanation for selective targeting of tumor cells by anti-CD47 approaches.

Rationale for novel anti-CD47/IO combinations
Since targeting CD47 results in activation of innate immunity, it follows that anti-CD47 strategies are likely to synergize with other immunotherapies, such as those which activate cytotoxic T cells. Recent work has illustrated that CD8+ T cells are necessary to elicit the therapeutic effect of CD47 antibodies in syngeneic tumor models (Figure 14). The cytosolic DNA sensor, STING, also appears to be critical for the CD47-mediated therapeutic effect in these models by mediating DC/macrophage antigen cross-presentation. It is therefore logical to expect synergism between anti-CD47 and IO agents that enhance T cell stimulation and antigen cross presentation such as anti-CTLA4, anti-PD1/L1, and STING agonists. Investors should soon get a glimpse of the potential for a CD47/IO cocktail as Trillium has announced plans to present data on preclinical IO combinations with their SIRPα-Fc lead molecule at this years annual ASH meeting.

Trillium Therapeutics SIRPα-Fc checkpoint inhibitor program
Trillium Therapeutics is targeting CD47 by using a soluble SIRPα decoy receptor which is fused to the Fc region of IgG, thus maintaining effector function of the molecule. The decoy fusion protein approach is differentiated from competitors using monoclonal antibodies raised against CD47. Although exact details surrounding the Trillium clinical candidate have not been divulged, the patent literature we’ve examined suggests that the Trillium approach could yield a molecule on the order of 80 kDa, which is significantly smaller than the 150 kDa size of the average IgG antibody. And for biologics, molecule size is directly proportional to tissue distribution. With a potentially smaller molecule, Trillium’s approach may be differentiated by way of having better tissue distribution. This could be particularly important when it comes to running solid tumor trials. Much like the data for anti-CD47 antibodies (Figure 13), the Trillium SIRPα-Fc selectively induces phagocytosis of tumor versus normal cells (shown in Figure 16). The potency of their lead molecules has been demonstrated in AML xenografts, where SIRPα-Fc administration results in the eradication of AML cells from immunocomprimised mice (Figure 17). In addition, chronic exposure of mice to a murine version of SIRPα-Fc does not result in disruption of normal hematopoietic parameters (Figure 16). Although, in this context, the definition of chronic is only four weeks; this does serve as an important data point in favor of a good preclinical safety profile.



Trillium Therapeutics SIRPα-Fc may have best-in-class RBC binding profile
A headline risk to this therapeutic modality lies in the relatively high level of CD47 expression on RBCs. The potential issue posed by drug-RBC binding is twofold. First, potential RBC depletion resulting from engagement via SIRPα-Fc would be particularly problematic in patients with hematologic malignancies, where anemia is a common byproduct of their disease. Next, drug-RBC binding could act as a SIRPα-Fc sink, altering the pharmacokinetic profile by reducing exposure and target engagement and ultimately negatively impacting efficacy. Although selectivity for tumor versus RBC phagocytosis has been demonstrated (see Figure 16), RBC binding still remains a valid concern as the company prepares to initiate clinical trials before years end. Trillium’s candidate selection process has been informed by the work of John Dick and colleagues, whereby they discovered SIRPα polymorphisms in NOD mice that modulate hematopoietic cell engraftment and RBC binding. This knowledge has allowed Trillium to purposely select low-RBC-binding SIRPα variants, which possess a lower intrinsic RBC binding capacity than many anti-CD47 monoclonal antibodies (Figure 18). The company reports show a RBC binding assay with a number of other CD47 mAbs, showing a multi-log difference between their lead and several antibodies. Although it isn’t immediately obvious, there is a competitor antibody included in this assay. 5F9 appears to be the Stanford clinical candidate (as described in a Stanford patent and clinical trial) and has on the order of 3 logs higher binding capacity to RBCs. Trillium’s markedly lower RBC binding profile may represent a competitive advantage over the Stanford antibody currently in clinical development (see Figure 21 for the CD47 competitive landscape). Though these data are incrementally positive for Trillium, caution should be used when extrapolating from an in vitro assay to potential adverse clinical outcomes.

Trillium management and scientific advisors
The recent addition of Eric Sievers as Chief Medical Officer should serve as a positive signal and, in our view, speaks to the future prospects of the company. Eric joined Trillium earlier this year from Seattle Genetics, where he worked as the Senior Vice President of Clinical Development. We’ll leave it up to the reader to interpret the implications of leaving a high-profile position from arguably the leader in oncology antibody-drug-conjugates, for a small, somewhat unknown Canadian biotechnology company. The intellectual property of Trillium is based on the research of John Dick. Dr. Dick is a household name in the leukemia field. He was the first to identify leukemic stem cells, and has pioneered the use of immunocomprimised mice to model human tumors. There is no doubt he is an invaluable voice on the Trillium scientific advisory board.

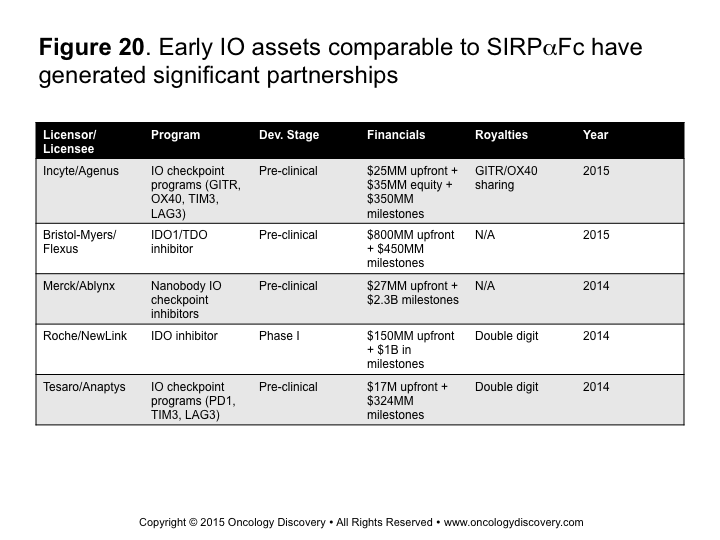
BioPharma is hungry for early-stage IO assets
It seems like deals involving immuno-oncology assets and/or the formation of new companies in this area are being announced on a daily basis. There is no doubt that all major oncology players have entered the immuno-oncology arena and are here to stay. They also most certainly have their business development units positioned to be acutely aware of new developments in this space. Positive and/or encouraging clinical data from Trillium or its competitors would likely trigger a favorable partnership from a larger IO player. See Figure 20 for recent partnership details on early stage IO assets.

The CD47 competitive landscape
The current front runner in this space is a monoclonal CD47 antibody program currently in development from Stanford. The discovery work, which led to the Stanford program was spearheaded by Irving Weissman; who, like John Dick, has focused much of his research efforts towards the study of stem cells. Dr. Weissman’s lab has no doubt been a major contributor to the CD47 cancer field. If you’re interested in Dr. Weissman’s work, Pubmed is a great place to start. Stanford currently has an ongoing phase I in patients with advanced solid malignancies, which is fully enrolled (see Figure 21 and here). August of 2017 is scheduled as the study completion date, but interim safety and efficacy updates are possible. Weissman and Majeti have recently published a characterization of their clinical candidate (Hu5F9-G4) in PLOS ONE (see here). Recall that Trillium’s SIRPα-Fc is differentiated from Hu5F9-G4 on the basis of a reduced RBC binding profile (see Figure 18).
In 2012 Celgene acquired a CD47 monoclonal antibody from Inhibrx for an undisclosed up-front payment, up to $500 million in milestones, and an undisclosed royalty rate. Their clinical candidate, CC-90002, has apparently been engineered to reduce RBC hemagglutination (see the Figures in their patent filing here) , but there are no data available to verify this claim. Their clinical candidate also has differentiated single agent efficacy as compared to Stanford’s candidate in a Raji lymphoma xenograft model (recall Figure 11 and characterization of the Stanford clinical candidate here). Celgene began enrollment of their phase I trial in February of this year in patients with advanced solid and hematological malignancies. Patients will receive the drug weekly via an IV fusion on a 28 day cycle. The study completion date is December 2017.
NovImmune, a small Swiss biotechnology company, is developing a bispecific anti-CD47/CD19 molecule that is currently in preclinical development. The bispecific approach is one also being taken by scientists at Stanford. Should either of these approaches advance to the clinic, their utility will be restricted to CD19+ liquid cancers like lymphoma, and will therefore not have the same broad utility as either CD47 monoclonal antibodies or SIRPα fusion proteins.

Trillium Therapeutics valuation
In order to assess the value of SIRPα-Fc, we employed a probability-adjusted multiple of sales analysis, assuming a 20% probability of success and modest market penetration in relapsed refractory acute myeloid leukemia as well as non-hodgkin lymphoma. We applied a 6X multiple on the US 2025E sales, using a 12% weighted average cost of capital. In our model, all ex-US sales, additional indications, and combination uses represent sources of upside to our valuation (see Figure 22 for details). This model values TRIL equity per share at $52.94, which represents a 3.5 fold upside to the current share price of $15.73.

Final thoughts
Trillium recently filed an IND for their SIRPα-Fc clinical candidate and expects to begin enrolling their phase I study in Q4 of 2015. Their study will seek to enroll lymphoma patients with normal hematological parameters to assess the hematological safety impact of their drug. After establishing an appropriate dose they plan on enrolling expansion cohorts of MDS and AML patients. Additional preclinical data on their SIRPα-Fc program is expected at ASH later this year.
Given the overwhelming supportive preclinical data, targeting the CD47-SIRPα axis in cancer is a therapeutic approach that deserves clinical prosecution. This novel therapeutic modality has broad potential across a range of hematologic and solid cancer types. The anticipated synergy between anti-CD47 agents and either targeted or novel IO therapies could allow for Trililum’s SIRPα-Fc to become a backbone of many oncology drug cocktails. To date, investing in Trillium Therapeutics represents the most compelling and attractive way to bet on the future promise of CD47 as an immuno-oncology target.
{kind=link}
if you have any questions or comments feel free to reach out to me on Twitter or via email at garrett@oncologydiscovery.com
Publicly traded companies mentioned: Trillium Therapeutics (TRIL), Seattle Genetics (SGEN)
Disclaimer: All opinions expressed on Oncology Discovery are my own and do not necessarily represent the position of my employer. The information presented within this article is not a solicitation for investment. We may have investments in mentioned companies.
Copyright © 2015 Oncology Discovery. All Rights Reserved. Unauthorized use and/or duplication of this material without permission is strictly prohibited.
Comments are closed.